
12-min read | Category: Ethics & Professional Practice | CE Credits Available
Professional Boundaries For Therapist most boundary violations that result in license discipline do not begin with a therapist intending harm. They begin with a gradual erosion — a small exception made once, a rationalization repeated until it becomes habit, a dual relationship allowed to drift past the point of return. Understanding professional boundaries is not about memorizing a list of prohibitions. It is about developing the clinical judgment to recognize when the therapeutic relationship is being compromised before a violation occurs.
This guide covers the Professional Boundaries For Therapist every licensed therapist, counselor, psychologist, and social worker should know — with practical frameworks, jurisdiction-specific considerations for clinicians in states with ethics CE requirements, and guidance on where to deepen your ethics training through continuing education.
Why Professional Boundaries For Therapist Exist — and What Happens When They Fail
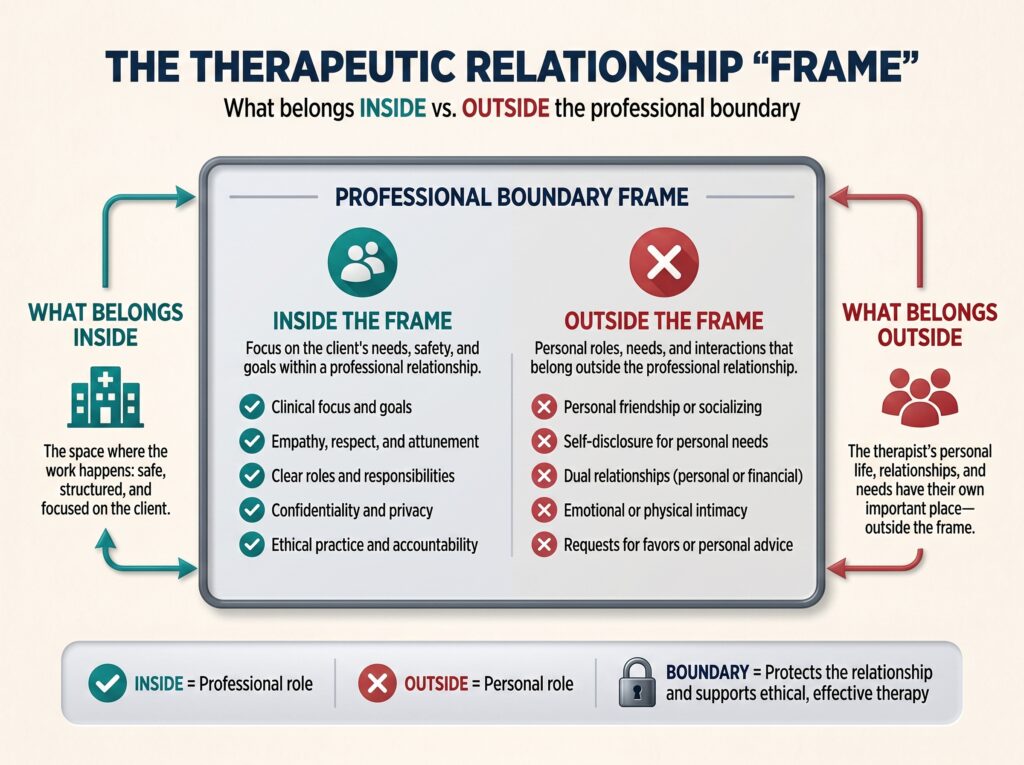
Professional Boundaries For Therapist define the limits of the therapeutic relationship. They exist to protect three things simultaneously: the client’s wellbeing and autonomy, the integrity of the therapeutic frame, and the therapist’s own professional standing and mental health.
When boundaries are violated, the consequences operate on multiple levels:
-
- For the client: exploitation, re-traumatization, loss of trust in help-seeking, harm to therapeutic gains
-
- For the therapist: licensing board complaints, civil liability, loss of licensure, professional isolation
-
- For the profession: erosion of public trust that affects every clinician’s ability to do their work
Licensing boards across the U.S. consistently list boundary violations — particularly dual relationships and sexual misconduct — among the leading causes of disciplinary action. The NASW Code of Ethics and the ACA Code of Ethics both devote extensive sections to boundary-related obligations, and familiarity with the specific code governing your licensure type is a baseline professional requirement.
Dual Relationships: The Most Clinically Complex Boundary
A dual relationship occurs when a therapist holds a second role with a client beyond the therapeutic one — as friend, employer, instructor, business partner, romantic partner, or community member in a close-knit setting. Not all dual relationships are equally problematic, and this is where many clinicians get into trouble: treating all dual relationships as either automatically acceptable or automatically prohibited, rather than evaluating each on its specific clinical and ethical merits.
When Dual Relationships Are Unavoidable
Rural and small-community practitioners face inherent dual relationship challenges — the client you see Monday morning may also be your child’s teacher or your neighbor. Therapists in these settings are not automatically in violation; they are navigating a structural reality. The ethical obligation is to manage the dual relationship actively rather than ignore it:
-
- Document the dual relationship and your reasoning at the outset
-
- Discuss the potential impact with the client directly
-
- Consult with a colleague or supervisor
-
- Establish clear agreements about how the roles will be kept separate
-
- Monitor for role confusion or exploitation risk throughout treatment
When Dual Relationships Become Violations
The clearest violations involve power differentials and exploitation:
-
- Sexual or romantic relationships with current clients — prohibited absolutely by every major ethics code
-
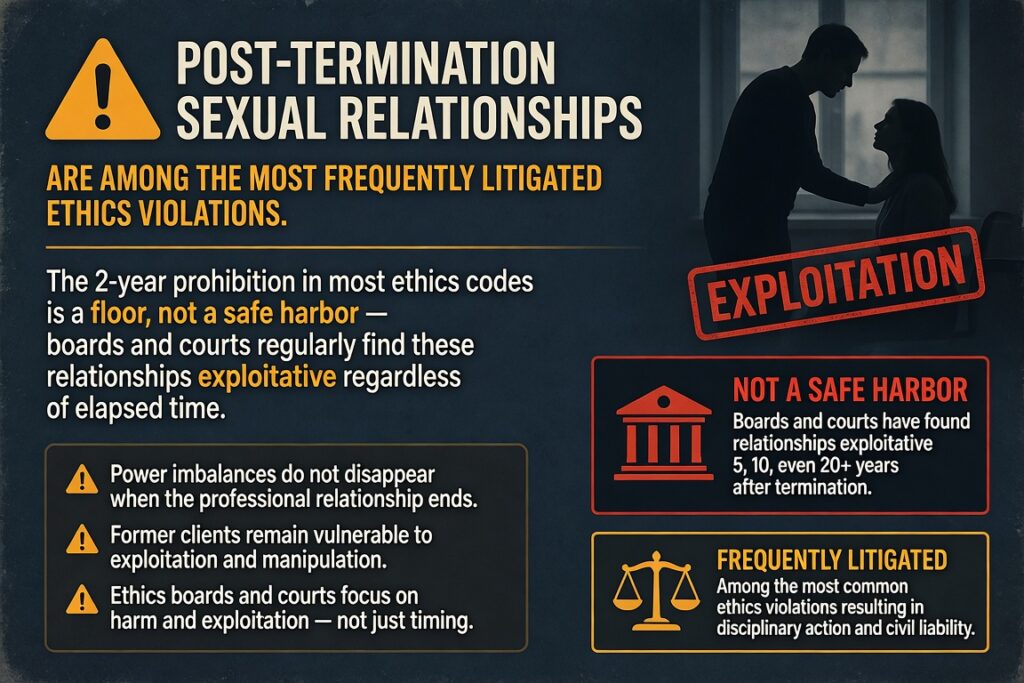
- Sexual relationships with former clients — prohibited for at least 2 years post-termination (ACA, APA) and considered exploitative in virtually all circumstances regardless of time elapsed
-
- Business relationships that compromise clinical judgment or create financial dependence
-
- Accepting gifts of significant value — context-dependent, but requires documentation and supervision consultation
-
- Bartering for therapy — only permissible when not clinically contraindicated, not exploitative, and entered into at the client’s initiative
Therapist Self-Disclosure: A Clinical Tool with Ethical Edges
Professional Boundaries For Therapist Self-disclosure is not inherently a boundary violation — used skillfully, it can deepen the therapeutic alliance, normalize client experience, and model vulnerability. The ethical question is not whether to self-disclose but whose needs the disclosure serves.
Clinically appropriate self-disclosure is:
-
- Brief and purposeful — not a therapist processing their own material
-
- Responsive to the client’s therapeutic goals
-
- Followed by a return of focus to the client
-
- Documented with clinical rationale in session notes
Inappropriate self-disclosure that crosses into boundary violation territory includes:
-
- Sharing personal struggles that shift the client into a caretaker role
-
- Disclosing political, religious, or lifestyle views unprompted in ways that could pressure the client
-
- Using the session to meet the therapist’s own social or emotional needs
-
- Continuing to share personal information after the client signals discomfort
The APA Ethical Principles of Psychologists address self-disclosure within the context of multiple relationships and client welfare. Full text: APA Ethics Code.
Digital and Social Media Boundaries: The New Ethics Frontier
Social media has created ethical terrain that no ethics code written before 2000 adequately addresses. The core principle — maintaining the integrity of the therapeutic relationship — applies, but the specific applications require deliberate policy and ongoing clinical attention.
Client Contact Through Digital Channels
-
- Social media friend/follow requests: Decline them. The overlap of personal and professional identity on social platforms compromises the therapeutic frame regardless of privacy settings.
-
- Therapist social media presence: Therapists who maintain a public professional presence (common for practice marketing) should have a clear policy about client contact and communicate it during informed consent.
-
- Texting and email: Only through HIPAA-compliant platforms when used for clinical communication. Policies should be established in writing during intake.
-
- Telehealth platforms: Must meet HIPAA security requirements. Using FaceTime or standard Zoom outside of a Business Associate Agreement is a compliance violation.
Searching Clients Online
Googling a client without their knowledge sits in ethically contested territory. Most ethics bodies advise against it outside of clear safety concerns, for several reasons:
-
- It introduces information into the therapeutic relationship that the client did not choose to share
-
- It can compromise the therapist’s neutrality
-
- It creates an asymmetry of knowledge that can subtly distort the therapeutic alliance
Where online searching is conducted (e.g., risk assessment situations), it should be disclosed to the client and documented.
Therapist Online Self-Presentation
A therapist’s public social media presence can inadvertently disclose values, lifestyle, and personal views that complicate the therapeutic frame for current or prospective clients. This does not mean therapists must be invisible online — but it does mean that digital self-presentation requires the same intentionality as in-person self-disclosure. The upcoming Clinical Events training Ethical Considerations of Technology, AI, and Social Media (June 27 | 3 Ethics CE Credits) addresses exactly these questions — including emerging issues around AI tools in clinical practice.
Confidentiality: Knowing Its Limits Is as Important as Keeping It
Confidentiality is the foundation of the therapeutic relationship — and clinicians who fail to understand its limits create as much risk as those who breach it carelessly. Clients need accurate informed consent about what is and is not confidential so they can make meaningful decisions about what to disclose.
The standard exceptions to confidentiality in U.S. clinical practice:
-
- Duty to warn / protect: Tarasoff obligations — varies by state. Some states mandate warning identifiable third parties; others permit it; some impose no duty. Know your state law.
-
- Imminent danger to self: Active suicidal ideation with plan, means, and intent typically triggers a duty to act — though the specific legal obligations vary by jurisdiction.
-
- Child abuse and neglect: Mandatory reporting applies to all licensed mental health professionals in all U.S. states. Know your state’s reporting threshold.
-
- Elder and dependent adult abuse: Mandatory reporting in most states.
-
- Court orders and subpoenas: A subpoena is not automatically an order to disclose — consult with an attorney before releasing records.
-
- HIPAA exceptions: Treatment, payment, healthcare operations, and specific public health/safety provisions.
New York Clinicians: State-Specific Ethics and CE Requirements
New York licensed mental health professionals — LCSWs, LMHCs, LMFTs, psychologists, and licensed mental health practitioners — are subject to New York Education Law and NYSED regulations in addition to federal HIPAA requirements. Key state-specific considerations:
-
- Ethics CE requirement: New York mandates coursework in professional ethics as part of license renewal for most mental health licensure categories.
-
- NY Mandated Reporter Law: New York requires all mental health professionals to report reasonable suspicion of child abuse — the threshold is lower than many clinicians assume.
-
- Duty to protect in NY: New York follows a permissive (not mandatory) Tarasoff standard — clinicians may disclose to protect identifiable third parties but are not legally required to.
-
- Telehealth across state lines: NY therapists providing services to clients physically located in other states must confirm they meet that state’s licensure requirements — this is a growing area of disciplinary risk post-pandemic.
For NY clinicians, ethics CE credits that directly address these obligations are not merely a compliance checkbox — they are a substantive risk management strategy. Clinical Events is accredited to provide CE credits for NY and most U.S. jurisdictions. See: Clinical Events Accreditations.
Informed Consent: The Boundary Document Most Therapists Under-Use
Robust informed consent is one of the most underutilized boundary protection tools in clinical practice. Most therapists have intake paperwork. Fewer use informed consent as an active, living document that is revisited at key clinical junctures.
A thorough informed consent process should address:
-
- Nature and limits of confidentiality — including all mandatory exceptions
-
- Therapist’s qualifications, theoretical orientation, and approach
-
- What clients can expect from the therapeutic process and its limitations
-
- Fee structure, cancellation policies, and billing practices
-
- Contact policies: how, when, and through what platforms the therapist is reachable
-
- Social media policy — explicitly stating the therapist will not accept friend requests or follow clients
-
- Telehealth policies if services are delivered remotely
-
- Emergency procedures and after-hours crisis resources
-
- Supervisor disclosure if the clinician is under supervision
Informed consent should be obtained in writing, stored in the clinical record, and revisited when the therapeutic frame changes materially — a new presenting issue, a switch to telehealth, a fee modification, or a change in supervision status.
Verbal-only informed consent is a documentation liability. If it is not in writing, for legal and licensing board purposes, it did not happen.
Recognizing Boundary Drift Before It Becomes a Violation
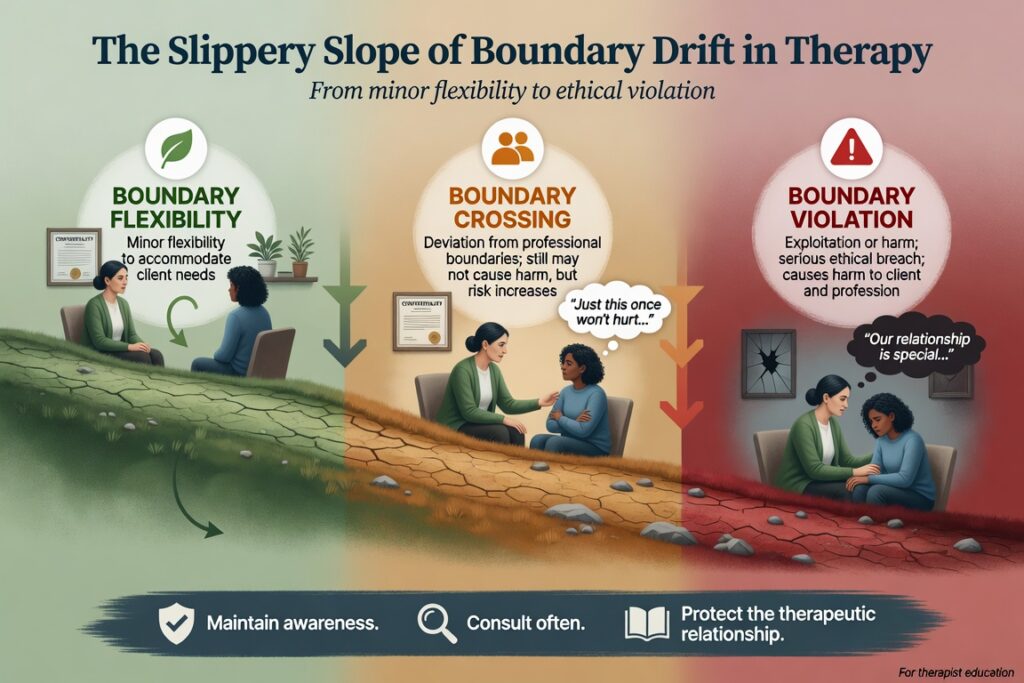
The concept of boundary drift — sometimes called the slippery slope in the ethics literature — describes the gradual, often unconscious process by which therapeutic boundaries erode over time. Individual exceptions seem reasonable in isolation; the cumulative effect is a compromised frame.
Warning signs that boundary drift may be occurring:
-
- Sessions running significantly over time with a specific client without clinical justification
-
- Reduced fee arrangements that are undocumented or emotionally rather than clinically motivated
-
- Sharing personal information outside of deliberate clinical self-disclosure
-
- Thinking about a client between sessions in a way that feels personal rather than clinical
-
- Dressing differently or preparing differently for sessions with a specific client
-
- Feelings of resentment, over-responsibility, or rescue urge toward a client
-
- Difficulty discussing a therapeutic relationship in supervision
When any of these signals appear, the appropriate response is immediate consultation or supervision — not rationalization. Most licensing board cases that end in disciplinary action began with boundary drift that the therapist recognized and did not act on.
Supervision and Peer Consultation: Your Primary Ethics Safeguard
The single most consistent predictor of ethical practice is not the therapist’s familiarity with ethics codes — it is their willingness to submit their clinical work to external scrutiny. Regular supervision and peer consultation create the accountability structure that prevents boundary drift from becoming boundary violation.
Ethically sound supervision and consultation practice:
-
- Maintain at least occasional peer consultation even post-licensure — formal requirements end but the clinical need does not
-
- Consult specifically when a therapeutic relationship feels unusual, when you notice strong countertransference, or when a client is pushing against the frame
-
- Document consultations in the clinical record — date, name of consultant, question posed, guidance received
-
- Participate in professional ethics trainings that expose you to case vignettes and ethical decision-making models, not just code memorization
The NASW Ethics resources and the APA Ethics Committee both publish case studies and advisory opinions that are invaluable for ongoing ethics education beyond CE requirements.
Ethics CE Credits Professional Boundaries For Therapist : Meet Your Requirement and Improve Your Practice
Ethics continuing education is mandatory in most U.S. states for license renewal — and the best ethics CE does more than satisfy a requirement. It builds the clinical judgment that protects clients, licenses, and the therapeutic relationship itself. Clinical Events offers accredited ethics CE credits specifically designed for licensed mental health professionals. Full accreditation details: Clinical Events Accreditations.
Upcoming ethics and professional practice CE trainings:
-
- Ethical Considerations of Technology, AI, and Social Media | June 27 | 3 Ethics CE Credits
-
- Ethics — Counseling in the Digital Age | August 22 | 3 Ethics CE Credits
-
- Motivational Interviewing Basics and Beyond | July 18 | 3 CE Credits — clinical skills with direct application to ethically complex client engagement
View all upcoming events: Clinical Events Training Calendar.
Frequently Asked Questions
Q1: What are professional boundaries in therapy?
Professional Boundaries For Therapist in therapy are the limits that define the therapeutic relationship and distinguish it from personal, social, or business relationships. They include physical limits (no sexual or romantic contact), relational limits (no dual relationships that could impair clinical judgment), communication limits (professional contact only through agreed channels), and self-disclosure limits (sharing personal information only when it serves the client’s therapeutic goals). Boundaries exist to protect client welfare, therapist integrity, and the efficacy of the therapeutic relationship.
Q2: What is a dual relationship in therapy and is it always a violation?
A dual relationship exists when a therapist holds more than one role with a client — as clinician and friend, clinician and employer, clinician and teacher. Not all dual relationships constitute ethics violations. In rural or small-community settings, some degree of role overlap may be unavoidable. The key ethical question is whether the secondary relationship impairs clinical judgment, exploits the client, or compromises the therapeutic frame. When it does — or risks doing so — the dual relationship is ethically prohibited.
Q3: Can a therapist be friends with a former client?
This is one of the most frequently asked boundary questions and one of the least definitively answered. Most ethics codes prohibit sexual or romantic relationships with former clients for a minimum of 2 years post-termination and consider them exploitative in virtually all circumstances even after that period. Social friendship is not explicitly prohibited by most codes, but it carries significant risk: the power differential established in the therapeutic relationship does not simply disappear at termination. Post-termination contact of any kind should involve careful ethical reflection, consultation, and documentation.
Q4: What are the limits of confidentiality therapists must disclose?
Therapists must inform clients during informed consent that confidentiality has several exceptions: imminent risk of harm to self or others, mandatory child abuse reporting, mandatory elder and dependent adult abuse reporting in most states, court orders for records, and certain HIPAA-permitted disclosures for treatment, payment, and healthcare operations. The specific legal obligations vary by state, and therapists have an ethical duty to know the laws in their jurisdiction and communicate them accurately to clients.
Q5: Do New York therapists have specific ethics CE requirements for license renewal?
Yes. New York State requires licensed mental health professionals — including LCSWs, LMHCs, LMFTs, and licensed psychologists — to complete continuing education that includes coursework in professional ethics as a condition of license renewal. NY therapists are also subject to state-specific obligations including mandatory reporting requirements, permissive Tarasoff duty-to-protect standards, and state telehealth regulations. For current NY requirements, see: NYSED Office of the Professions — Mental Health Practitioners. Clinical Events is accredited to provide ethics CE credits applicable to NY licensure renewal.
Q6: What should a therapist do if they suspect they have crossed a boundary?
Stop and consult — immediately. The worst response to a recognized boundary concern is rationalization or continued drift. The appropriate steps are: (1) Seek consultation or supervision to evaluate the situation from an outside perspective. (2) Review the relevant ethics code provisions for your licensure. (3) Document your awareness of the concern and the consultation in the clinical record. (4) If a violation has occurred, consult with a mental health attorney before taking further action. Early intervention almost always produces better outcomes — for the client and for the therapist — than delayed recognition.
Q7: Where can therapists earn ethics CE credits online?
Clinical Events offers live virtual ethics CE trainings accredited for therapists, counselors, psychologists, and social workers across the U.S. The Ethical Considerations of Technology, AI, and Social Media (June 27 | 3 Ethics CE Credits) and Ethics — Counseling in the Digital Age (August 22 | 3 Ethics CE Credits) are specifically designed to address the most current professional boundary challenges facing clinicians today. View full offerings at clinicalevents.org/events.
No comment yet, add your voice below!