
11-min read | Category: Generalized Anxiety Disorder | CE Credits Available
Generalized Anxiety Disorder (GAD) is one of the most common presentations in outpatient mental health settings — and one of the most frequently undertreated. The reason is not a shortage of effective interventions. The research base for GAD is robust. The problem is that chronic worry is often normalized, both by clients and by clinicians, until the disorder has profoundly eroded quality of life.
This guide covers the current evidence-based landscape for GAD treatment — what works, what the emerging models add, and where the clinical complexities lie — with practical takeaways for therapists at every experience level.
Understanding GAD: More Than Just Worry
GAD is characterized by persistent, excessive anxiety and worry about multiple domains — work, health, finances, relationships — that is difficult to control and accompanied by somatic symptoms such as muscle tension, fatigue, difficulty concentrating, irritability, and sleep disturbance. Per DSM-5, symptoms must be present for at least six months and cause significant functional impairment.
What distinguishes GAD clinically from everyday stress or subclinical anxiety is not simply the presence of worry, but its pervasiveness, uncontrollability, and the way it generalizes across life domains. Clients often describe an inability to “turn off” their minds — a feature that has important implications for treatment target selection.
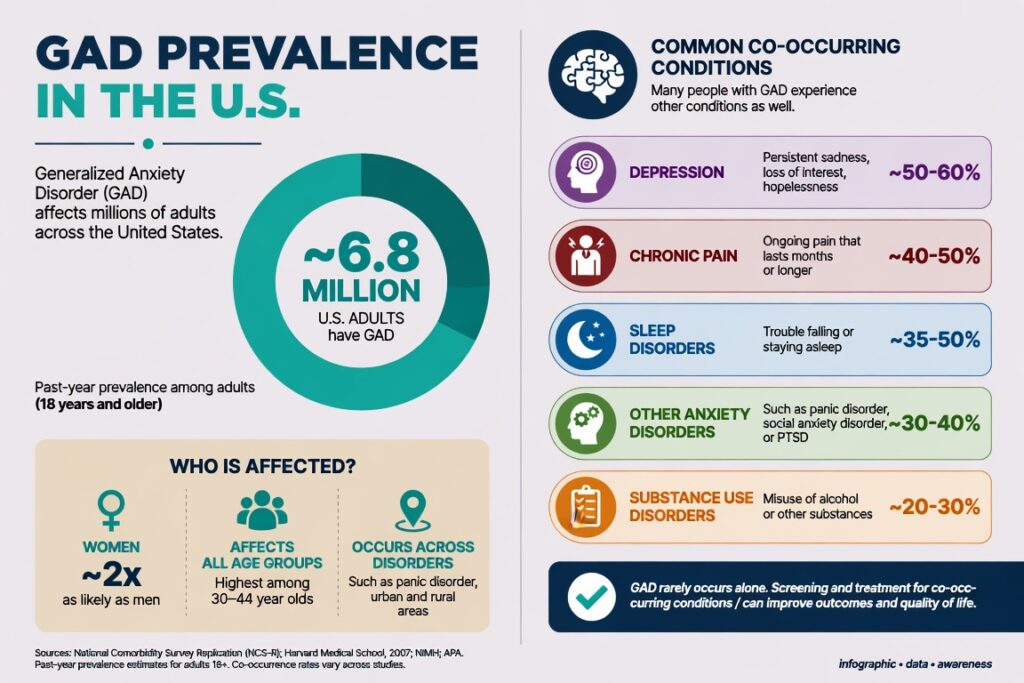
GAD has a lifetime prevalence of approximately 5.7% in the U.S. and is significantly more common in women. It frequently co-occurs with depression, other anxiety disorders, and chronic pain. For epidemiological data, see NIMH: Generalized Anxiety Disorder.
The Diagnostic Challenge: What Clinicians Often Miss
GAD is frequently misdiagnosed or missed entirely for two reasons: its somatic presentations lead clients to primary care rather than mental health settings, and its symptoms overlap substantially with depression, making differential diagnosis genuinely difficult.
Key diagnostic considerations:
- GAD worry tends to be future-oriented and pervasive; depressive rumination tends to be past-oriented and theme-specific
- Rule out medical contributors: hyperthyroidism, cardiac arrhythmia, substance use, medication side effects
- Assess for trauma history — hypervigilance can present similarly to GAD and requires a different primary treatment target
- Use validated measures at intake and to track progress: GAD-7, Penn State Worry Questionnaire (PSWQ), Hamilton Anxiety Rating Scale (HAM-A)
The American Psychological Association’s Clinical Practice Guidelines provide diagnostic decision trees and evidence ratings for anxiety disorder interventions.
Evidence-Based Treatments for GAD
1. Cognitive Behavioral Therapy (CBT) — The First-Line Standard
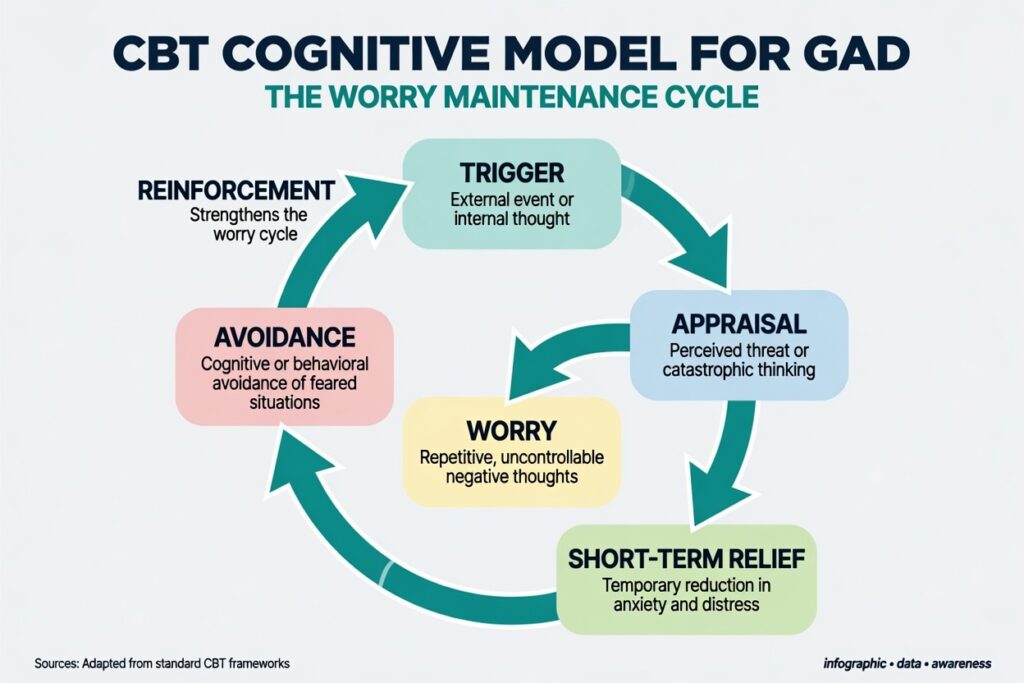
CBT remains the most extensively researched psychotherapy for GAD, with meta-analyses consistently showing large effect sizes versus waitlist and active comparisons. The classic CBT model targets two interconnected processes:
- Cognitive restructuring — identifying and challenging overestimations of threat probability and catastrophic thinking
- Behavioral engagement — reducing safety behaviors and avoidance that maintain the anxiety cycle
Core CBT components for GAD:
- Psychoeducation on the anxiety cycle and function of worry
- Cognitive restructuring targeting probability overestimation and catastrophizing
- Scheduled worry time — containing worry to a designated period rather than throughout the day
- Problem-solving training for realistic concerns
- Progressive muscle relaxation (PMR) and applied relaxation
- Behavioral experiments to test anxious predictions
CBT for GAD is typically delivered in 12–15 sessions, though research supports briefer formats (8–10 sessions) for milder presentations. The upcoming Clinical Events training Treating Social Anxiety, GAD, Panic, OCD, and PTSD (July 25 | 6 CE Credits) provides hands-on training in CBT protocols across the anxiety spectrum.
2. Acceptance and Commitment Therapy (ACT)
ACT represents a significant development in anxiety treatment. Rather than challenging the content of anxious thoughts, ACT targets the client’s relationship to those thoughts through psychological flexibility — the capacity to persist in valued behavior regardless of what the mind is producing.
The six ACT core processes applied to GAD:
- Acceptance — willingness to experience anxiety without fighting it
- Defusion — creating distance from worried thoughts rather than treating them as literal
- Present-moment awareness — reducing future-oriented rumination through contact with now
- Self-as-context — observing anxious experience without identification
- Values clarification — identifying what matters most as a guide to action
- Committed action — building behavior patterns in service of values despite anxiety
ACT and CBT show comparable effect sizes for GAD in head-to-head trials. ACT may be particularly useful for clients who have found thought challenging alienating or who show high levels of experiential avoidance. Many clinicians now integrate ACT flexibility processes with CBT’s cognitive precision.
3. Metacognitive Therapy (MCT)
MCT, developed by Adrian Wells, targets not the content of worry but the beliefs about worry itself — what Wells calls metacognitions. In GAD, clients typically hold two types of problematic metacognitive beliefs:
- Positive metacognitions: ‘Worrying keeps me safe,’ ‘If I worry, I’ll be prepared’
- Negative metacognitions: ‘My worry is uncontrollable,’ ‘Worrying will harm me’
MCT uses techniques such as postponing worry, attention training, and detached mindfulness to modify these metacognitive beliefs rather than the worried thoughts themselves. Controlled trials show MCT outperforming CBT on some outcomes, with faster symptom reduction in several studies — though the evidence base is smaller and replication is ongoing.
For clinicians wanting to explore MCT, the Wells Metacognitive Therapy Institute provides training resources.
4. Intolerance of Uncertainty (IU) Model
Research by Dugas, Robichaud, and colleagues identified intolerance of uncertainty (IU) — a dispositional inability to accept that the future is unpredictable — as a central maintaining factor in GAD. This model has strong empirical support and offers a focused treatment approach:
- Psychoeducation on the role of uncertainty in worry
- Behavioral experiments exposing clients to uncertain situations without reassurance-seeking
- Problem-orientation training
- Cognitive re-evaluation of the utility of worry
The IU model is particularly useful for clients who recognize their worry is irrational but cannot stop because of what might happen. It targets the intolerance itself rather than the content of catastrophic thoughts.
5. Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT)
Both MBSR and MBCT have demonstrated significant anxiety reduction in GAD populations. These approaches train sustained, non-judgmental present-moment awareness — directly countering the future-oriented mental time travel that characterizes GAD worry.
MBCT, originally developed for depression relapse prevention, has been adapted for anxiety and integrates CBT cognitive components with formal mindfulness practices. It is particularly well-suited for clients with comorbid depression and GAD — a common presentation.
For research on mindfulness interventions in anxiety, see NCCIH: Mind and Body Practices for Anxiety.
Combined Treatment: Psychotherapy and Pharmacotherapy
For moderate-to-severe GAD, combined treatment — psychotherapy plus medication — consistently outperforms either alone. First-line pharmacological options established in the literature include SSRIs (escitalopram, paroxetine) and SNRIs (venlafaxine, duloxetine), with buspirone as an anxiolytic alternative.
Therapists in outpatient settings should:
- Screen for current medication use and discuss potential interactions with psychotherapy (e.g., benzodiazepines can blunt the arousal needed for effective exposure work)
- Coordinate with prescribers around treatment targets and progress
- Be conversant with side effect profiles that clients may attribute to therapy outcomes
- Recognize that medication may lower the floor but therapy builds the ceiling — clients on medication alone have higher relapse rates than those who complete CBT
For prescribing guidelines and medication evidence summaries, see ADAA: Generalized Anxiety Disorder Treatment (Anxiety and Depression Association of America).
Clinical Complicators: When GAD Doesn’t Respond as Expected
Several factors predict poorer treatment response and require clinical attention:
Comorbid Depression
Comorbid MDD is present in approximately 60% of GAD cases. Depression typically needs to be addressed concurrently, as it suppresses the behavioral activation necessary for anxiety reduction. Integrated CBT protocols targeting both conditions simultaneously outperform sequential treatment.
Chronic Worry as Identity
Long-standing GAD clients often have incorporated worry into their self-concept as responsibility, conscientiousness, or preparation. Challenging worry directly can feel like an attack on character. Motivational interviewing techniques at the outset can reduce ambivalence and improve engagement.
Medical Comorbidities
GAD frequently co-occurs with IBS, chronic pain, cardiovascular conditions, and autoimmune disorders — often in a bidirectional relationship. Clinicians should resist the urge to treat GAD in isolation and coordinate with medical providers where somatic symptoms are prominent.
Trauma Underpinning
Trauma history is common in GAD populations and may require primary trauma treatment before anxiety-focused work proceeds effectively. For clinicians working at this intersection, see the Clinical Events training Treating Social Anxiety, GAD, Panic, OCD, and PTSD which addresses the diagnostic and treatment overlaps across multiple anxiety presentations.
A Practical Treatment Planning Framework for GAD
Rather than selecting a single modality, skilled GAD treatment integrates components based on the individual client’s profile:
- Step 1 — Assessment: GAD-7, PSWQ, IU Scale, trauma screen, functional impairment
- Step 2 — Psychoeducation: Anxiety cycle, function of worry, treatment rationale
- Step 3 — Stabilization: PMR, diaphragmatic breathing, sleep hygiene
- Step 4 — Core Intervention: CBT cognitive restructuring + behavioral experiments OR ACT defusion/values work, depending on client fit
- Step 5 — Targeted Modules: IU-focused exposure, metacognitive restructuring, mindfulness integration
- Step 6 — Relapse Prevention: Early warning sign identification, maintenance strategies, booster session plan
Progress should be tracked with the GAD-7 at each session — not just at intake and termination. Lack of improvement by session 4–6 should prompt reassessment of diagnosis, treatment fit, and engagement quality.
Expand Your Anxiety Treatment Competence with CE Credits
Treating GAD effectively requires more than familiarity with the CBT model. Clinicians need hands-on skill-building in protocol delivery, case conceptualization, and managing the presentations that don’t follow the textbook. Clinical Events offers accredited live virtual CE trainings designed specifically for licensed mental health professionals. See full accreditation details at Clinical Events Accreditations.
Upcoming trainings directly relevant to anxiety treatment:
- Treating Social Anxiety, GAD, Panic, OCD, and PTSD | July 25 | 6 CE Credits
- Motivational Interviewing Basics and Beyond | July 18 | 3 CE Credits — essential for engagement-resistant GAD clients
- Addressing Compassion Fatigue: Evidence-Based Strategies for Helpers | August 29 | 3 CE Credits
Browse the full training calendar: All Upcoming Clinical Events.
Frequently Asked Questions
Q1: What is the most effective therapy for Generalized Anxiety Disorder?
CBT has the largest and most replicated evidence base for GAD and is considered the first-line psychotherapy. ACT and Metacognitive Therapy (MCT) show comparable or in some studies superior results. The most effective therapy for any individual client depends on their specific maintaining factors — intolerance of uncertainty, cognitive fusion, or metacognitive beliefs about worry — and clinician competence in the chosen modality.
Q2: How many therapy sessions does it take to treat GAD?
Standard CBT protocols for GAD run 12–15 sessions, with briefer formats (8–10 sessions) supported for milder presentations. ACT and MCT can show effects in as few as 8–12 sessions. Comorbid depression, long duration of illness, or significant functional impairment typically requires longer treatment. Progress monitoring with the GAD-7 every session is the best guide to treatment length.
Q3: Is GAD a lifelong condition?
GAD tends toward a chronic, fluctuating course if untreated — but it is highly treatable. Research shows that CBT produces substantial improvement in 50–60% of clients, with many achieving full remission. Relapse prevention work at the end of treatment significantly reduces recurrence. GAD should not be framed to clients as a permanent condition requiring indefinite management.
Q4: What is intolerance of uncertainty and how does it relate to GAD?
Intolerance of uncertainty (IU) refers to a negative dispositional response to uncertain situations regardless of their probability or impact. In GAD, IU functions as a core maintaining process — clients worry as a strategy to feel prepared for all possible outcomes, even when the probability of negative events is low. Treatment approaches targeting IU directly focus on building tolerance for uncertainty through behavioral experiments rather than reassurance-seeking.
Q5: How is GAD treated differently from panic disorder or social anxiety?
GAD involves pervasive, multi-domain worry without a specific trigger, whereas panic disorder centers on fear of physical sensations and social anxiety on feared negative evaluation. While all three benefit from CBT, the specific targets differ: GAD treatment focuses on the worry process and intolerance of uncertainty; panic treatment centers on interleroceptive exposure; social anxiety treatment emphasizes social behavioral experiments and attention retraining. Clinicians treating multiple anxiety presentations benefit from comprehensive cross-disorder training.
Q6: Where can therapists earn CE credits for GAD and anxiety disorder treatment?
Clinical Events offers accredited live virtual CE training on anxiety disorders, including the July 25 session Treating Social Anxiety, GAD, Panic, OCD, and PTSD (6 CE Credits), designed specifically for licensed therapists, counselors, psychologists, and social workers.


2 Comments
It is perfect time to make some plans for the future and it’s time to
be happy. I’ve read this post and if I could I desire to suggest you some interesting things or suggestions.
Perhaps you can write next articles referring to this article.
I want to read more things about it!
Great content! Keep up the good work!