
Trauma affects millions of people every year, yet no single therapeutic approach works equally well for every client. While some individuals respond positively to structured cognitive interventions, others continue experiencing symptoms despite understanding their trauma intellectually. This reality has encouraged many clinicians to explore both traditional and body-based treatment approaches when developing trauma-informed care plans.
One of the most common questions therapists ask is whether Somatic Therapy vs CBT for Trauma offers better outcomes for specific client populations. The answer depends on several factors, including the client’s trauma history, nervous system regulation, emotional awareness, cognitive abilities, and treatment goals.
Understanding the strengths and limitations of both approaches allows clinicians to make more informed treatment decisions while providing individualized care. Rather than viewing these therapies as competing models, many trauma specialists now recognize that they can complement one another when used appropriately.
As trauma research continues to evolve, clinicians are gaining a deeper understanding of how traumatic experiences affect both the brain and the body. Advances in neuroscience have shown that trauma is not stored solely as memories or thoughts; it can also be reflected in physiological responses, muscle tension, autonomic nervous system activation, and patterns of emotional regulation. This growing body of evidence has expanded interest in body-based interventions while reinforcing the value of established cognitive approaches.
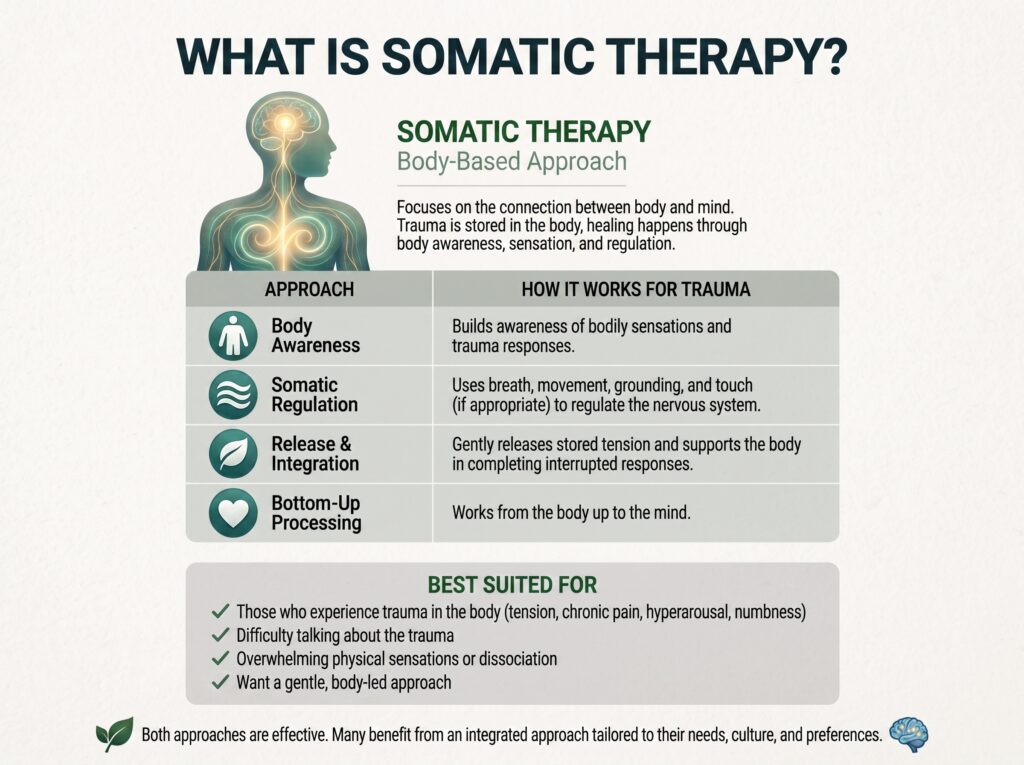
Somatic Therapy is a body-oriented approach to psychotherapy that focuses on the connection between physical sensations, emotions, and traumatic experiences. Rather than concentrating only on thoughts and beliefs, somatic interventions help clients become aware of how trauma is experienced within the body.
Many individuals living with trauma experience symptoms such as chronic muscle tension, hypervigilance, sleep disturbances, emotional numbness, or persistent feelings of being “stuck.” These reactions often reflect nervous system dysregulation rather than conscious choices. Somatic Therapy seeks to restore regulation by helping clients safely notice bodily sensations, complete interrupted defensive responses, and gradually increase their capacity to tolerate emotional experiences.
Common techniques used in Somatic Therapy include:
- Body awareness exercises
- Breath regulation
- Grounding techniques
- Movement-based interventions
- Mindfulness practices
- Nervous system regulation strategies
- Pendulation and titration techniques
- Interoceptive awareness
Many modern trauma models incorporate somatic principles, including Somatic Experiencing®, Sensorimotor Psychotherapy, Polyvagal-informed interventions, and elements of Internal Family Systems (IFS). These approaches emphasize safety, pacing, and the therapeutic relationship while helping clients reconnect with their bodies after trauma.
Somatic Therapy may be particularly beneficial for clients experiencing:
- Complex PTSD
- Developmental trauma
- Dissociation
- Panic symptoms
- Chronic anxiety
- Emotional dysregulation
- Trauma stored as physical tension
- Persistent nervous system activation
Research supported by organizations such as the National Center for PTSD and the National Institute of Mental Health (NIMH) continues to highlight the importance of understanding trauma through both neurological and physiological perspectives. These findings reinforce the growing role of body-based interventions as part of comprehensive trauma treatment.
However, Somatic Therapy is not intended to replace cognitive interventions in every situation. Instead, many clinicians view it as one valuable component within a broader trauma-informed treatment plan. Choosing the most appropriate intervention depends on each client’s clinical presentation, treatment readiness, and therapeutic goals.
In the next section, we’ll examine Cognitive Behavioral Therapy (CBT) and explore why it remains one of the most researched and widely used evidence-based approaches for treating trauma and PTSD.
What Is Cognitive Behavioral Therapy (CBT)?
Cognitive Behavioral Therapy (CBT) is one of the most extensively researched and widely practiced forms of psychotherapy for trauma, anxiety, depression, and post-traumatic stress disorder (PTSD). Unlike body-oriented therapies, CBT focuses primarily on identifying and modifying unhelpful thoughts, beliefs, and behavioral patterns that contribute to emotional distress.
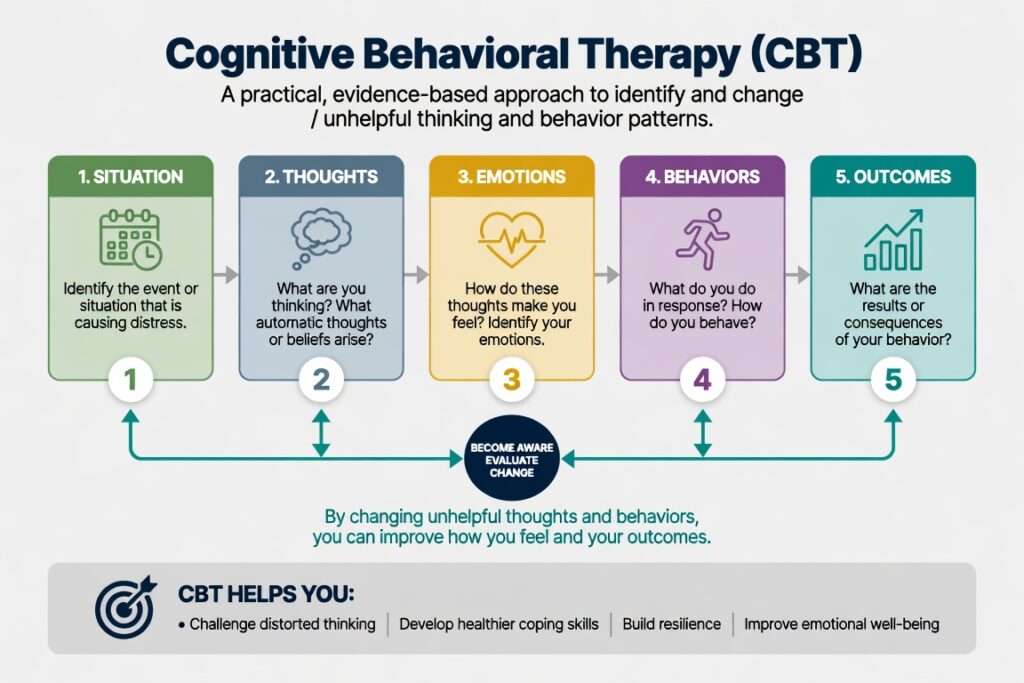
The foundation of CBT is based on the idea that our thoughts, emotions, and behaviors are interconnected. Following a traumatic experience, many clients develop automatic negative beliefs such as:
- “I’m not safe.”
- “The trauma was my fault.”
- “I can’t trust anyone.”
- “I’ll never recover.”
These cognitive distortions can reinforce fear, avoidance, shame, and hopelessness. CBT helps clients recognize these patterns, challenge inaccurate beliefs, and replace them with healthier, evidence-based thinking.
Common CBT techniques include:
- Cognitive restructuring
- Exposure-based interventions
- Behavioral activation
- Thought records
- Problem-solving skills
- Coping skills training
- Relaxation techniques
- Homework assignments between sessions
Trauma-focused CBT (TF-CBT) is particularly effective for children, adolescents, and adults experiencing PTSD symptoms after traumatic events. The American Psychological Association (APA) recognizes trauma-focused CBT as one of the evidence-based treatments for PTSD.
For therapists interested in current trauma treatment guidelines, the APA Clinical Practice Guideline for PTSD provides an excellent overview:
Similarly, the National Center for PTSD, operated by the U.S. Department of Veterans Affairs, offers extensive clinician resources on evidence-based trauma therapies.
Somatic Therapy vs CBT for Trauma: Key Differences
Understanding Somatic Therapy vs CBT for Trauma is less about determining which approach is “better” and more about identifying which intervention best aligns with a client’s clinical needs.
While both therapies aim to reduce trauma symptoms and improve overall functioning, they approach healing from different perspectives.
| Somatic Therapy | Cognitive Behavioral Therapy (CBT) |
| Focuses on the body’s response to trauma | Focuses on thoughts and behaviors |
| Helps regulate the nervous system | Helps restructure negative thinking |
| Uses body awareness and physical sensations | Uses cognitive exercises and behavioral strategies |
| Particularly useful for dysregulation and dissociation | Particularly useful for distorted beliefs and avoidance |
| Bottom-up processing | Top-down processing |
| Emphasizes felt experience | Emphasizes cognitive understanding |
Many trauma specialists now recommend integrating both approaches rather than viewing them as competing models.
For example, a client experiencing panic attacks, hyperarousal, and chronic muscle tension may first benefit from somatic regulation techniques before engaging in cognitive restructuring exercises.
Conversely, a client primarily struggling with catastrophic thinking and avoidance behaviors may initially respond well to CBT interventions before incorporating body-based practices.
The conversation around Somatic Therapy vs CBT for Trauma continues to evolve as neuroscience demonstrates that trauma affects both cognitive processing and physiological regulation.
Which Clients Benefit Most from Somatic Therapy?
Although every client is unique, research suggests that certain populations may particularly benefit from body-oriented interventions.
Somatic Therapy is often recommended for clients who experience:
Complex PTSD
Individuals with prolonged interpersonal trauma frequently experience chronic nervous system dysregulation that extends beyond cognitive symptoms.
Dissociation
Clients who disconnect from their emotions or physical sensations may gradually rebuild body awareness through carefully paced somatic interventions.
Developmental Trauma
Early attachment disruptions often become deeply embedded within physiological regulation patterns, making body-based work especially valuable.
Chronic Hypervigilance
Clients who constantly feel “on guard” may learn to regulate their autonomic nervous system through grounding and body awareness exercises.
Emotional Numbing
Some trauma survivors intellectually understand their experiences but struggle to reconnect emotionally.
Somatic approaches help bridge that gap by increasing awareness of internal bodily sensations.
Increasingly, clinicians are combining somatic methods with Polyvagal Theory, mindfulness, and Internal Family Systems (IFS) to create comprehensive trauma-informed treatment plans.
Clinicians interested in expanding these skills may benefit from specialized continuing education focused on trauma integration.
Healing Complex PTSD & Dissociation with an Integrative Model
This training explores practical applications of somatic therapies alongside IFS, EMDR, and Polyvagal Theory for complex trauma treatment.
Which Clients Benefit Most from CBT?
CBT remains one of the strongest evidence-based approaches for many trauma presentations.
Clients often benefit most when they:
- Experience intrusive thoughts
- Engage in avoidance behaviors
- Struggle with anxiety disorders
- Experience depression alongside trauma
- Hold persistent negative self-beliefs
- Need structured treatment plans
- Prefer logical, skills-based approaches
CBT is particularly effective when clients are ready to examine and challenge maladaptive thinking patterns.
For example, individuals experiencing persistent guilt or self-blame after trauma often make significant progress through cognitive restructuring techniques.
Similarly, clients with specific phobias or avoidance behaviors frequently benefit from gradual exposure exercises conducted within a safe therapeutic environment.
The National Institute of Mental Health (NIMH) provides additional evidence regarding cognitive therapies for PTSD and trauma-related disorders.
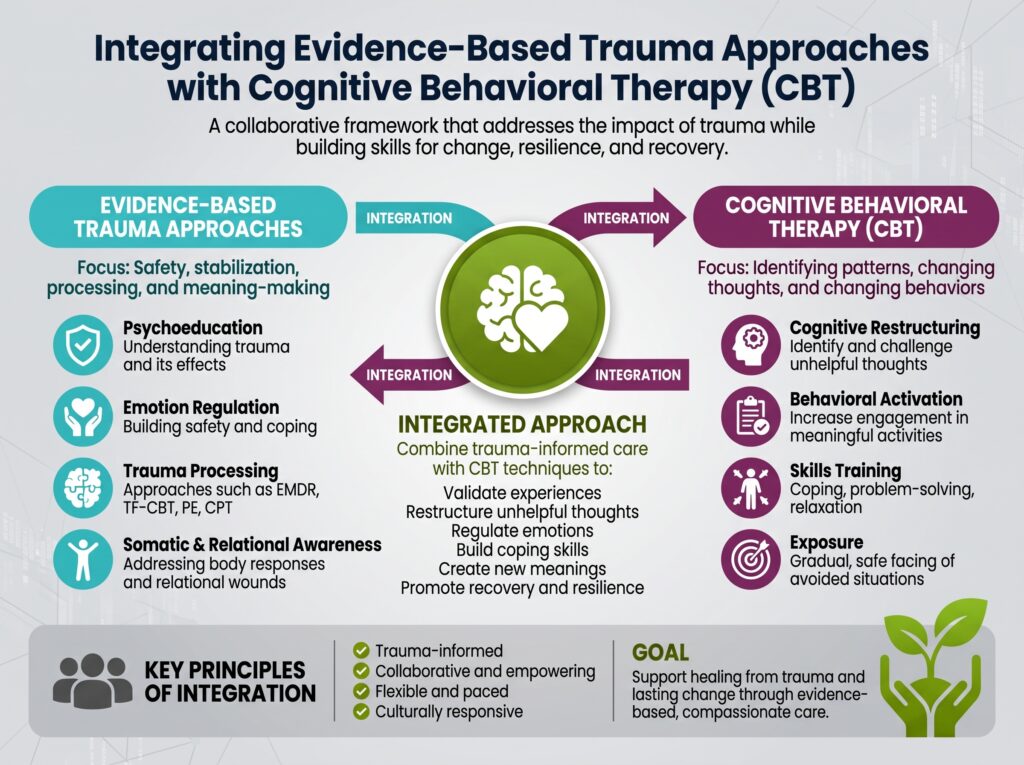
Integrating Evidence-Based Trauma Approaches
Rather than asking whether Somatic Therapy vs CBT for Trauma is superior, many experienced clinicians now ask:
“Which intervention does this particular client need at this particular stage of recovery?”
This shift reflects the growing recognition that trauma treatment is rarely one-size-fits-all. Effective clinicians draw from multiple evidence-based modalities, adapting their approach to the client’s symptoms, strengths, and readiness for change.
Continue Expanding Your Clinical Skills
At Clinical Events, we provide evidence-based continuing education designed to help therapists integrate emerging trauma treatments into everyday practice.
Explore upcoming CE trainings related to trauma, neuroscience, and evidence-based psychotherapy:
- Upcoming CE Events: https://clinicalevents.org/events/
- Clinical Events Blog: https://clinicalevents.org/blog/
- Provider Approvals & Accreditations: https://clinicalevents.org/accreditations/
Can Somatic Therapy and CBT Be Combined?
The discussion surrounding Somatic Therapy vs CBT for Trauma often suggests that therapists must choose one approach over the other. However, current trauma research and clinical experience indicate that many clients benefit most from an integrative treatment plan that combines both body-based and cognitive interventions.
Trauma affects multiple systems simultaneously. It influences thoughts, emotions, behaviors, relationships, memory, and the autonomic nervous system. Because trauma is multidimensional, treatment often requires more than a single therapeutic modality.
For example, a client may first need somatic interventions to regulate chronic hyperarousal before they are emotionally available for cognitive restructuring. Once their nervous system feels safer, CBT techniques can help challenge distorted beliefs and reinforce healthier coping strategies.
Similarly, clients who begin treatment with CBT may later discover unresolved physiological responses that continue triggering anxiety, panic, or dissociation. Incorporating somatic techniques at that stage can deepen recovery and improve long-term outcomes.
Rather than asking which therapy is superior, clinicians increasingly ask:
- What symptoms are most impairing today?
- Is the client emotionally regulated enough for cognitive work?
- Does the client remain chronically dysregulated despite cognitive insight?
- Which intervention will improve safety, engagement, and treatment readiness?
These questions encourage individualized care instead of rigid adherence to a single therapeutic model.
Current Research and Evidence
Over the past two decades, trauma research has significantly expanded our understanding of how psychological trauma affects both the brain and body.
Organizations such as the American Psychological Association (APA) recognize trauma-focused CBT as one of the strongest evidence-based treatments for PTSD.
The National Center for PTSD, operated by the U.S. Department of Veterans Affairs, also recommends several evidence-based trauma therapies while emphasizing individualized treatment planning.
Meanwhile, neuroscience research has demonstrated that traumatic experiences frequently alter autonomic nervous system functioning, emotional regulation, and physiological responses.
The National Institute of Mental Health (NIMH) provides additional information regarding PTSD, trauma recovery, and emerging research into effective interventions.
Similarly, the Substance Abuse and Mental Health Services Administration (SAMHSA) promotes trauma-informed care principles that prioritize safety, trustworthiness, collaboration, empowerment, and cultural responsiveness.
Collectively, these organizations reinforce an important clinical message:
Effective trauma treatment is individualized, evidence-informed, and responsive to each client’s unique presentation.
Continuing Education Helps Therapists Deliver Better Trauma Care
Trauma treatment continues to evolve rapidly. New research surrounding Polyvagal Theory, attachment, neuroscience, Internal Family Systems (IFS), EMDR, and somatic interventions is changing how clinicians conceptualize recovery.
For therapists, ongoing professional development is essential for remaining current with these advances.
Clinical Events offers live continuing education trainings designed specifically for mental health professionals seeking practical, evidence-based skills.
If you’re interested in expanding your trauma-informed practice, consider these upcoming trainings:
Healing Complex PTSD & Dissociation with an Integrative Model
Learn practical applications of:
- Internal Family Systems (IFS)
- EMDR
- Somatic Therapies
- Polyvagal Theory
Working with Developmental Trauma and Attachment from a Somatic Lens
Explore body-based interventions that strengthen attachment-focused trauma treatment.
Explore More Clinical Resources
Visit the Clinical Events Blog for additional evidence-based articles covering trauma, neuroscience, ethics, CBT, DBT, motivational interviewing, and continuing education.
Conclusion
When comparing Somatic Therapy vs CBT for Trauma, the evidence suggests that the question should not be which therapy is universally better, but rather which approach best meets the client’s current needs.
CBT remains one of the most researched and effective interventions for addressing maladaptive thoughts, avoidance behaviors, and PTSD symptoms. Somatic Therapy complements these strengths by targeting nervous system regulation, body awareness, and physiological responses that often persist after trauma.
For many clients, combining both approaches provides the most comprehensive path toward healing.
As our understanding of trauma continues to evolve, clinicians who integrate evidence-based cognitive techniques with body-oriented interventions are often better equipped to provide individualized, compassionate, and effective care.
Investing in ongoing education allows therapists to confidently apply these emerging approaches while improving outcomes for the individuals and families they serve.
Frequently Asked Questions
1. What is the main difference between Somatic Therapy and CBT for trauma?
Somatic Therapy focuses on how trauma is stored and experienced within the body, emphasizing nervous system regulation and body awareness. CBT primarily addresses thoughts, beliefs, and behaviors that contribute to emotional distress. Both approaches can be effective depending on the client’s clinical needs.
2. Which therapy is better for Complex PTSD?
Many clinicians find that clients with Complex PTSD benefit from an integrative approach. Somatic interventions may improve emotional regulation and body awareness, while CBT can help address unhelpful thinking patterns and avoidance behaviors.
3. Can Somatic Therapy and CBT be used together?
Yes. Many trauma-informed therapists combine Somatic Therapy and CBT to address both physiological regulation and cognitive restructuring. The combination often provides a more comprehensive treatment plan.
4. Is CBT considered an evidence-based treatment for PTSD?
Yes. Trauma-focused Cognitive Behavioral Therapy is recognized by organizations such as the American Psychological Association and the National Center for PTSD as an evidence-based treatment for PTSD.
5. Who benefits most from Somatic Therapy?
Clients experiencing chronic nervous system dysregulation, dissociation, developmental trauma, emotional numbing, or persistent physical symptoms related to trauma may benefit from Somatic Therapy.
6. Why is continuing education important for trauma therapists?
Trauma research continues to evolve rapidly. Continuing education helps therapists remain current with emerging evidence-based approaches, improve clinical decision-making, and better support diverse client populations.
7. Where can therapists learn more about evidence-based trauma treatment?
Clinical Events offers live continuing education programs focused on trauma, neuroscience, attachment, ethics, and integrative psychotherapy.
8. Where can I find trusted information about PTSD treatment?
Authoritative U.S.-based resources include:
- American Psychological Association (APA): https://www.apa.org/
- National Institute of Mental Health (NIMH): https://www.nimh.nih.gov/
- National Center for PTSD: https://www.ptsd.va.gov/
- SAMHSA: https://www.samhsa.gov/

No comment yet, add your voice below!