
12-min read | Category: Trauma & PTSD | CE Credits Available
Published by Clinical Events
Reviewed by Stacy Ruse, LPC, ERYT-500
Treat Complex PTSD
Most clinicians learned PTSD treatment through the lens of a single-incident trauma. But Complex PTSD (C-PTSD) — born from repeated, prolonged trauma often beginning in childhood — requires a fundamentally different clinical approach. The standard 8-session protocol simply does not hold.
This guide breaks down what the research actually supports for treating C-PTSD, which modalities are gaining traction, and how therapists can expand their trauma competence through structured continuing education.
What Makes Complex PTSD Different from Classic PTSD
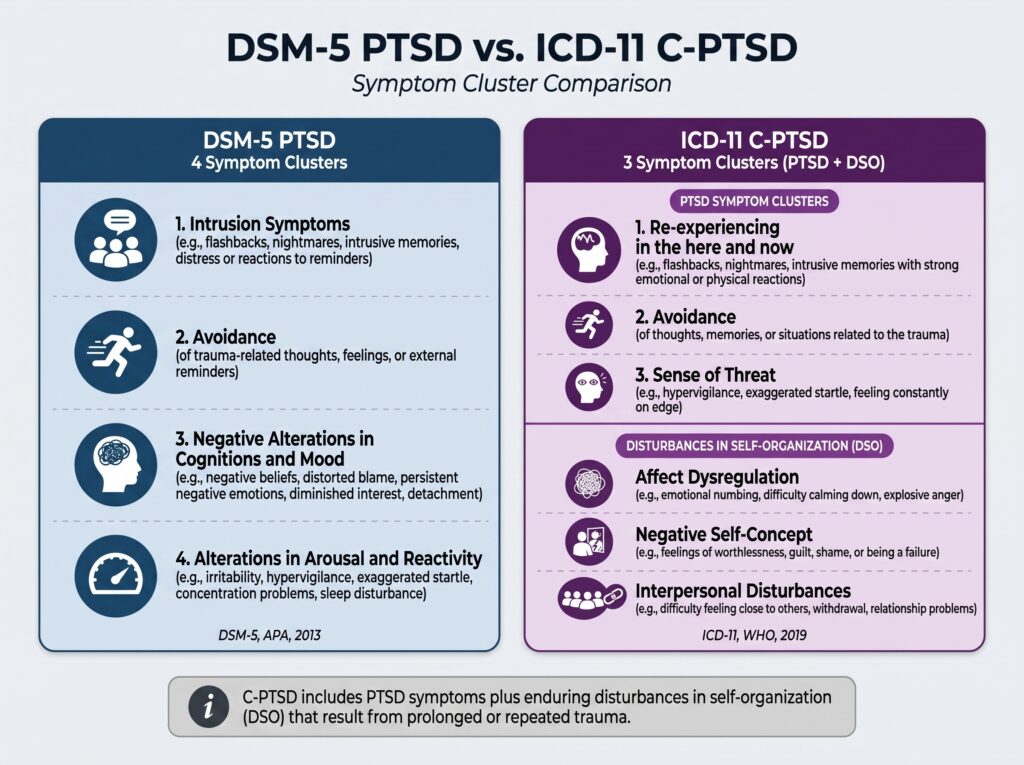
C-PTSD was formally recognized in the ICD-11 (2019) as a distinct diagnosis. It shares the core PTSD symptom cluster — reexperiencing, avoidance, and hyperarousal — but adds three additional disturbances of self-organization (DSO):
- Affect dysregulation — difficulty modulating emotional responses
- Negative self-concept — pervasive shame, guilt, and feelings of worthlessness
- Disturbances in relationships — difficulty trusting others, chronic interpersonal conflict
Importantly, the DSM-5 does not include C-PTSD as a standalone diagnosis. Clinicians in the U.S. typically code it under PTSD with additional specifiers or comorbid diagnoses (e.g., Persistent Depressive Disorder, Borderline Personality Disorder). Understanding this diagnostic gap is essential — it shapes insurance authorization, treatment planning, and client psychoeducation. For a deeper clinical discussion, see PTSD Treatment Guidelines from the American Psychological Association.
Why Standard PTSD Protocols Often Fail with Complex Trauma
Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT) — both first-line treatments for PTSD — show weaker outcomes for C-PTSD populations. A key reason: these protocols assume a stable enough window of tolerance to process traumatic memory. Many C-PTSD clients lack that stability at the outset.
Throwing a complex trauma survivor into trauma-focused processing before building adequate stabilization can lead to:
- Emotional flooding and decompensation
- Premature termination of therapy
- Reinforcement of the client’s belief that healing is impossible
The SAMHSA National Center for Trauma-Informed Care notes that trauma-informed practice must account for the pervasive impact of trauma across all body systems, not just memory — a principle standard PTSD protocols frequently underweigh. See: SAMHSA Trauma-Informed Approach.
Evidence-Based Approaches for Treating Complex PTSD
1. Phase-Based Treatment (The Gold Standard Framework)
The International Society for Traumatic Stress Studies (ISTSS) recommends a phased treatment approach for complex trauma as its primary guideline. The three phases are:
- Phase 1 — Safety, stabilization, and skill-building
- Phase 2 — Trauma processing and integration
- Phase 3 — Consolidation and reconnection
This is not a rigid sequence — clients move back and forth between phases. The therapist’s job is to track window of tolerance and titrate accordingly. Full ISTSS guidelines are available at ISTSS Treatment Guidelines.
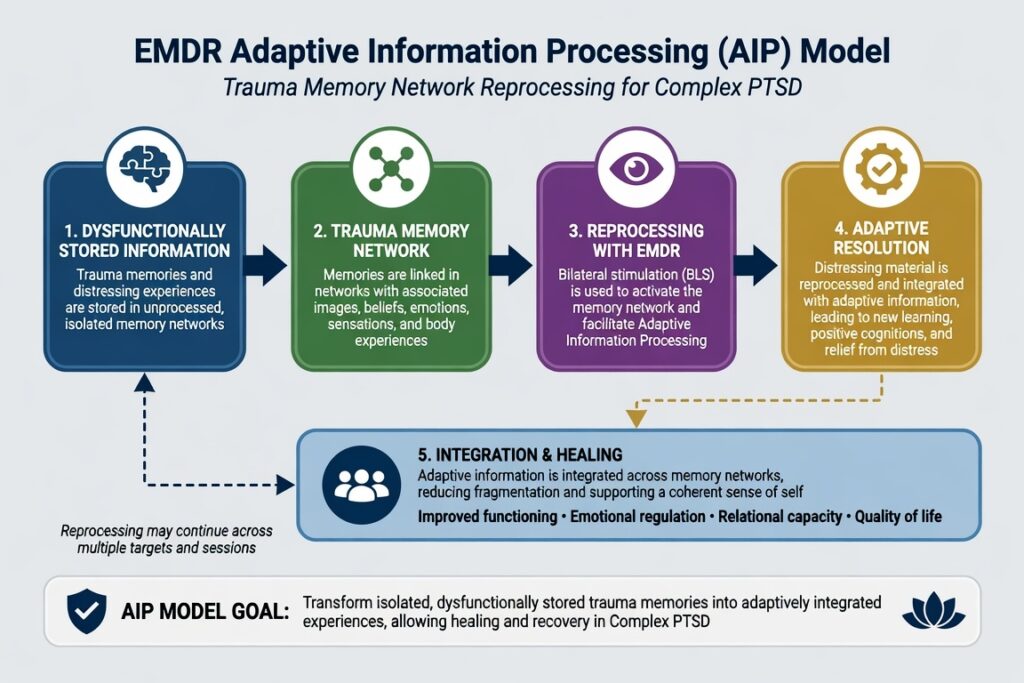
2. EMDR (Eye Movement Desensitization and Reprocessing)
EMDR has strong evidence for standard PTSD and growing support for C-PTSD when delivered with careful phase-1 preparation. For complex trauma, the protocol typically involves extended stabilization (resource installation, safe place) before any reprocessing begins.
Key adaptations for C-PTSD:
- Longer Phase 2 (history taking) to map trauma networks
- Resource Development and Installation (RDI) for regulation
- Slow, titrated processing — avoiding full abreaction
The EMDR International Association (EMDRIA) offers clinician training, consultation groups, and research resources.
3. Internal Family Systems (IFS)
IFS, developed by Richard Schwartz, conceptualizes the psyche as a system of “parts” — exiles (wounded young parts carrying trauma burdens), managers (protective parts), and firefighters (reactive parts). For C-PTSD clients, this model offers a non-pathologizing, parts-based framework that aligns well with the fragmented self-experience characteristic of complex trauma.
IFS is gaining recognition in trauma treatment literature, though large-scale RCTs remain limited. It is particularly useful for clients with dissociative features, extreme shame, and rigid protective systems that block standard trauma processing.
4. Somatic and Body-Based Approaches
Bessel van der Kolk’s foundational work established that trauma is stored in the body — a premise now embedded in several evidence-informed modalities:
- Somatic Experiencing (SE) — Peter Levine’s model focusing on body sensation and pendulation
- Sensorimotor Psychotherapy — integrating body awareness with attachment and cognitive work
- Trauma-Sensitive Yoga — as an adjunct to verbal therapy
Clinical Events features a dedicated training on somatic approaches: Working with Developmental Trauma and Attachment from a Somatic Lens (August 15 | 3 CE Credits).
5. Trauma-Focused CBT (TF-CBT) — Adapted for Adults
Originally developed for children, TF-CBT principles have been adapted for adult complex trauma. Core components include psychoeducation, relaxation, affective modulation, cognitive coping, trauma narrative, and enhancing safety. The cognitive restructuring components are particularly useful for addressing the pervasive negative self-concept seen in C-PTSD.
For a broader CBT framework covering PTSD, anxiety, and OCD, see the upcoming Clinical Events training: Treating Social Anxiety, GAD, Panic, OCD, and PTSD (July 25 | 6 CE Credits).
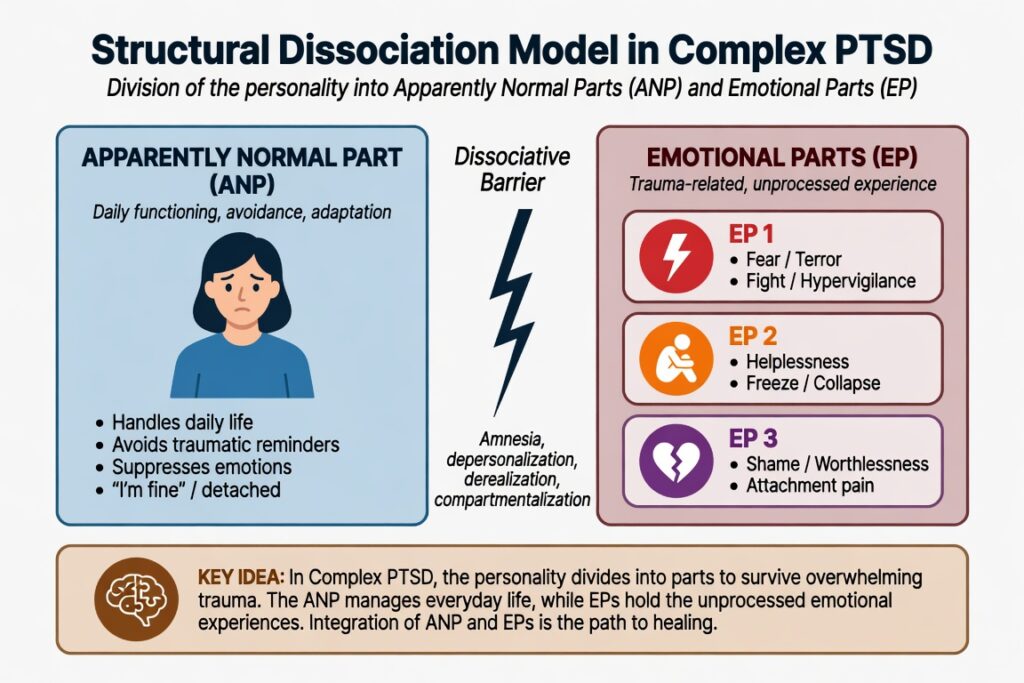
The Role of Dissociation in Treat Complex PTSD Treatment
Dissociative symptoms are common in C-PTSD and represent one of the primary clinical complicators. The Structural Dissociation of the Personality model (Onno van der Hart et al.) describes how traumatic experience fragments the personality into an Apparently Normal Part (ANP) and Emotional Parts (EPs).
Clinicians must screen for dissociation before beginning trauma processing. Proceeding without addressing dissociation risks destabilizing clients and reinforcing fragmentation rather than integration.
Screening tools to consider:
- Dissociative Experiences Scale (DES)
- Multiscale Dissociation Inventory (MDI)
- Somatoform Dissociation Questionnaire (SDQ-20)
Clinical Events addresses these clinical complexities directly in the July 11 training: Healing Complex PTSD & Dissociation (3 CE Credits) — highly recommended for any clinician working with C-PTSD populations.
Therapeutic Relationship as a Treatment Mechanism
In C-PTSD treatment, the therapeutic relationship is not merely the container for technique — it is itself a primary mechanism of change. Repeated relational trauma creates attachment injuries that only heal through corrective relational experience.
Key relational competencies for complex trauma work:
- Consistent attunement and repair of ruptures
- Transparency about the therapeutic process
- Explicit attention to transference and countertransference
- Recognition of how power dynamics within therapy can replicate early trauma
This is precisely why burnout and compassion fatigue are occupational hazards in trauma work. Clinical Events offers targeted CE training on this issue: Addressing Compassion Fatigue: Evidence-Based Strategies for Helpers (August 29 | 3 CE Credits).
Building Competence in Complex Trauma: CE Credit Opportunities
Complex PTSD is not a specialty you develop from reading alone. Supervised clinical work, consultation, and structured continuing education are all required for genuine competence.
Clinical Events provides live virtual CE trainings specifically designed for therapists, counselors, psychologists, and social workers working with trauma populations. All programs are accredited — see full details on the Clinical Events Accreditations page.
Upcoming trauma-relevant CE trainings:
- July 11: Healing Complex PTSD & Dissociation | 3 CE Credits
- July 25: Treating Social Anxiety, GAD, Panic, OCD, and PTSD | 6 CE Credits
- August 15: Working with Developmental Trauma and Attachment from a Somatic Lens | 3 CE Credits
- August 29: Addressing Compassion Fatigue | 3 CE Credits
View the full calendar: All Upcoming Clinical Events.
(FAQ)
Q1: What is the most effective treatment for Complex PTSD?
No single modality is definitively superior. The ISTSS recommends a phase-based framework — prioritizing stabilization before trauma processing — as the overarching structure. Within that structure, EMDR, IFS, somatic approaches, and adapted CBT all have meaningful evidence. The best treatment is one matched to the client’s current window of tolerance and relational capacity.
Q2: Is Complex PTSD in the DSM-5?
No. C-PTSD was formally recognized in the ICD-11 (2019) but has not been added to the DSM-5 or DSM-5-TR. U.S. clinicians typically diagnose under PTSD with additional specifiers or identify comorbid conditions (e.g., BPD, MDD) that capture the full clinical picture.
Q3: How is C-PTSD different from Borderline Personality Disorder (BPD)?
This remains a clinically contested distinction. Both diagnoses involve affect dysregulation, relational difficulties, and identity disruption. The key differentiators in ICD-11 C-PTSD are a clear trauma etiology and the absence of some BPD features (e.g., impulsivity, self-harm as a defining feature, frantic efforts to avoid abandonment). Many clinicians argue for a trauma-informed reconceptualization of BPD itself rather than sharp differentiation.
Q4: Can EMDR be used with Complex PTSD clients?
Yes, with important modifications. Standard EMDR protocol requires adequate stabilization before reprocessing. For C-PTSD clients, this means extended Phase 1 work — often many sessions building resources, affect regulation skills, and stabilization — before any trauma-focused processing begins. Clinicians should pursue advanced EMDR training and consultation specifically in complex trauma applications.
Q5: How long does treatment for Complex PTSD typically take?
Significantly longer than standard PTSD treatment. Research suggests 2–4 years of therapy is common for individuals with severe C-PTSD, though outcomes vary substantially based on severity, co-occurring conditions, social support, and therapeutic fit. Setting realistic expectations with clients at the outset — without communicating hopelessness — is a critical early therapeutic task.
Q6: Where can therapists earn CE credits for complex trauma training?
Clinical Events offers accredited live virtual CE trainings on complex trauma, dissociation, somatic approaches, and related topics. The July 11 training Healing Complex PTSD & Dissociation is specifically designed for mental health professionals seeking to expand their trauma competence while fulfilling CE requirements.
Looking to build confidence treating Complex PTSD?
Join our live virtual CE training:
Healing Complex PTSD & Dissociation with an Integrative Model
✅ Earn 3 CE Credits
✅ Live Virtual Training

No comment yet, add your voice below!